Tanima Jana1, Jennifer Shroff2, Manoop S Bhutani3
1 Department of Internal Medicine, University of Texas Medical School at Houston, Houston, TX, USA
2 Department of Internal Medicine, Division of Gastroenterology, Hepatology and Nutrition, University of Texas Medical School at Houston, Houston, TX, USA
3 Department of Gastroenterology, Hepatology and Nutrition, The University of Texas MD Anderson Cancer Center, Houston, TX, USA
| Date of Submission | 22-Dec-2014 |
| Date of Acceptance | 01-Feb-2015 |
| Date of Web Publication | 14-Mar-2015 |
Correspondence Address:
Manoop S Bhutani
Department of Gastroenterology, Hepatology and Nutrition, The University of Texas MD Anderson Cancer Center, Houston, TX
USA
Source of Support: None, Conflict of Interest: None
Pancreatic cystic lesions are being detected with increasing frequency, largely due to advances in cross-sectional imaging. The most common neoplasms include serous cystadenomas, mucinous cystic neoplasms, intraductal papillary mucinous neoplasms, solid pseudopapillary neoplasms, and cystic pancreatic endocrine neoplasms. Computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS) are currently used as imaging modalities. EUS-guided fine needle aspiration has proved to be a useful diagnostic tool, and enables an assessment of tumor markers, cytology, chemistries, and DNA analysis. Here, we review the current literature on pancreatic cystic neoplasms, including classification, diagnosis, treatment, and recommendations for surveillance. Data for this manuscript was acquired via searching the literature from inception to December 2014 on PubMed and Ovid MEDLINE.
Keywords: Cystic pancreatic endocrine neoplasm, endoscopic ultrasound, endosonography, intraductal papillary mucinous neoplasm, mucinous cystic neoplasm, pancreatic cystic neoplasms, serous cystic neoplasm, solid pseudopapillary neoplasm
How to cite this article:
Jana T, Shroff J, Bhutani MS. Pancreatic cystic neoplasms: Review of current knowledge, diagnostic challenges, and management options. J Carcinog 2015;14:3
How to cite this URL:
Jana T, Shroff J, Bhutani MS. Pancreatic cystic neoplasms: Review of current knowledge, diagnostic challenges, and management options. J Carcinog [serial online] 2015 [cited 2021 Oct 13];14:3. Available from: https://carcinogenesis.com/text.asp?2015/14/1/3/153285
Introduction
Pancreatic cystic neoplasms (PCN) comprise 10-15% of all pancreatic cystic lesions and approximately 1% of pancreatic neoplasms. [1],[2],[3],[4],[5] PCN can broadly be divided into mucinous lesions, including intraductal papillary mucinous neoplasms (IPMN) and mucinous cystic neoplasms (MCN), and nonmucinous lesions, which encompass serous cystic neoplasms (SCN), solid pseudopapillary neoplasms (SPN), and cystic pancreatic endocrine neoplasms (CPEN). [1],[6],[7],[8] In the Western hemisphere, the majority of PCN are serous cystadenomas (SCA) (32-39%), MCN (10-45%), and IPMN (21-33%). [6],[9] Symptomatic patients with PCN may present with jaundice, chronic abdominal pain, and recurrent pancreatitis (if obstruction is present), along with nonspecific symptoms of back pain, weight loss, anorexia, nausea, and vomiting. [8]
Imaging
Pancreatic cysts can be assessed with multiple imaging modalities, including CT and MRI, but these techniques are inconsistent, with variable accuracy ranging from 20% to 80%. [10] While endoscopic ultrasound (EUS) provides quality images, it has relatively low sensitivity and specificity in differentiating mucinous from nonmucinous cystic lesions, noted to be 56% and 45%, respectively, in one study. [11] Multiple studies have suggested positron emission tomography (PET-CT) to have a sensitivity of 92-100%, specificity of 87-100%, and accuracy of 94-96% in distinguishing benign from malignant IPMN. [12],[13],[14] However, due to higher cost, possible false negative results in borderline areas, and possible false positive results in areas of post-biopsy changes and pancreatitis, there is not sufficient data to support the routine use of PET-CT in this manner. [15]
Cyst Fluid Studies
Endoscopic ultrasound-guided cyst aspiration can be used to assist in diagnosis through the evaluation of cytology, tumor markers (carcinoembryonic antigen [CEA], carbohydrate antigen [CA] 72-4, CA 19-9), amylase, and DNA analysis [Table 1].
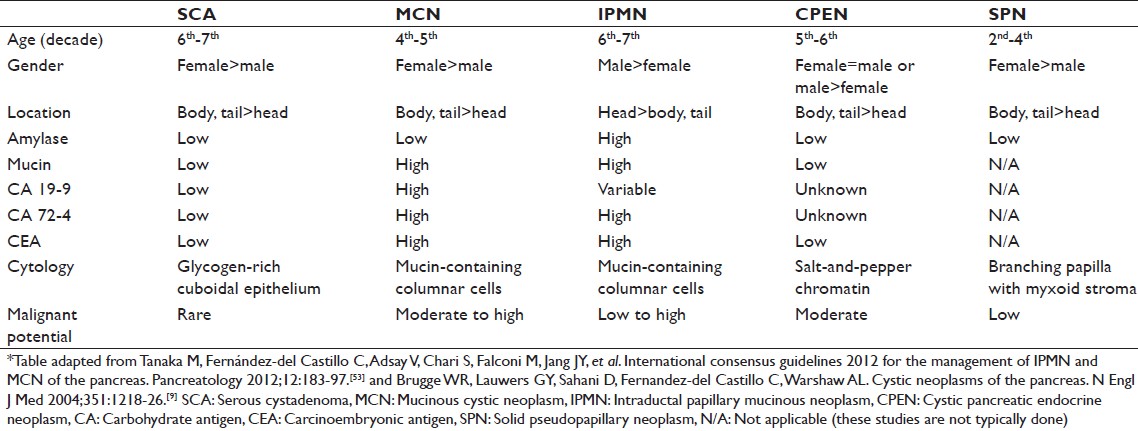 |
Table 1: Characteristics of pancreatic cystic neoplasms Click here to view |
Cytology
Cytology generally tends to show a high specificity but low sensitivity for detection of malignancy or differentiating mucinous from nonmucinous lesions. In a study of 45 patients, Moparty et al. obtained a sensitivity and specificity of 100% and 89%, respectively, for the detection of malignancy with EUS-guided fine needle aspiration (FNA). [2] However, other studies have reported sensitivities of only 27-50%. [16],[17] For the distinction of mucinous from nonmucinous lesions with cytology, studies have shown sensitivity of 35-43%, specificity of 83-96%, and accuracy of 58-59%. [11],[18]
Carcinoembryonic Antigen
Cyst fluid CEA level is considered the most accurate tumor marker for diagnosis of mucinous cystic lesions. [19] However, there is controversy over the appropriate cut-off for CEA levels. In a study of 442 patients, Snozek et al. concluded that an optimal cut-off was 30 ng/mL, with values >30 ng/mL revealing 79% sensitivity, 73% specificity, and 84% positive predictive value (PPV) for diagnosis of MCN. [20] In a study of 450 patients, van der Waaij et al. revealed that CEA levels below 5 ng/mL suggested a SCA or pseudocyst (PC) with 50% sensitivity and 95% specificity. [21] A CEA level <4 ng/mL has been shown to have a 100% sensitivity and 93% specificity for differentiating SCA from mucinous cystadenomas (MCA), mucinous cystadenocarcinomas (MCAC), and PC. [22] The Cooperative Pancreatic Cyst Study reported that a CEA cut-off of ≥192 ng/mL had a 73% sensitivity, 84% specificity, and 79% accuracy in distinguishing mucinous from nonmucinous lesions. [11] A CEA level ≥480 ng/mL combined with viscosity >1.6 has also been shown to accurately predict mucinous cysts. [10] Higher levels of CEA (i.e. >800 n/mL) have revealed 94% PPV, 98% specificity, 48% sensitivity, and 79% accuracy in differentiating MCA or MCAC from SCA or PC. [21] One limitation of CEA is that although a high CEA level may predict the presence of a mucinous lesion, it cannot distinguish between MCN versus IPMN. [7] In addition, CEA cannot be used to distinguish between malignant and benign IPMN lesions. [23] However, the study by Snozek et al. suggested that CA 19-9 level of <8000 U/mL with a CEA ≥30 ng/mL can be helpful in the diagnosis of IPMN. [20]
Amylase
The presence of amylase in a cyst is indicative of communication with the pancreatic duct (PD), and thus, SCA and MCA often have low amylase levels. [7] Cyst fluid amylase levels <250 U/L have been shown to have sensitivity of 44% and specificity of 98% in diagnosis of either SCA, MCA, or MCAC, and can be used to exclude PC. [21] While high levels of amylase are seen in IPMN, one study has shown that cyst fluid amylase levels cannot be used to distinguish MCN from branch-duct (BD)-IPMN. [24]
Carbohydrate Antigen 19-9 and Carbohydrate Antigen 72-4
A study of 113 patients utilizing a CA 19-9 cut-off value of >50,000 U/mL to distinguish mucinous cysts from other cystic lesions showed a 15% sensitivity and 81% specificity but an 86% sensitivity and 85% specificity in differentiating cystadenocarcinoma from other cystic lesions. [25] A CA 19-9 level<37 U/mL has shown a 98% specificity in detection of a PC or SCA, but only 19% sensitivity and 46% accuracy. [21] A CA 72-4 level>40 U /mL has been shown to have a 63% sensitivity and 98% specificity in distinguishing MCA and MCAC from SCA and PC. [22]
DNA Analysis
In the PANDA study, there was a specificity of 96% but only 37% sensitivity for the presence of malignancy in a cyst with the presence of a high-amplitude KRAS mutation, followed by allelic loss in cyst fluid. [26] An optimal approach may be combining CEA levels with molecular analysis, with one study reporting 100% sensitivity in the differentiation of mucinous from nonmucinous cysts. [27] One study has investigated the combination of KRAS and GNAS testing. In cases of IPMN, 66% contained a GNAS mutation, 81% KRAS, and 51% both GNAS and KRAS. With MCN, 33% contained KRAS mutations and none had any GNAS mutations. No GNAS or KRAS mutations were found in SCA. [28] In the same study, combining GNAS and KRAS mutations from cyst fluid showed a sensitivity of 96% and specificity of 100% in distinguishing IPMN from SCA, with no SCAs having either mutation. [28] MicroRNA and cytokines are also being explored in the evaluation of PCN. [19]
Needle-Based Confocal Laser Endomicroscopy
Needle-based confocal laser endomicroscopy (nCLE) is an emerging technique performed during EUS-FNA that allows real-time imaging of the internal structures of pancreatic cystic lesions. In the INSPECT pilot study, Konda et al. showed that nCLE has a sensitivity of 59%, specificity of 100%, PPV of 100%, and negative predictive value (NPV) of 50% when used to identify PCN based on the presence of epithelial villous structures. [29] In the CONTACT study by Napoléon et al., a superficial vascular network pattern was used to identify SCA with a sensitivity of 69%, specificity of 100%, PPV of 100%, NPV of 82%, and accuracy of 87%. [30]
Serous Cystic Neoplasms
Serous cystadenomas are benign, slow-growing tumors that are most common in women (75%) [7],[31] in the sixth decade of life. [6],[32] They account for approximately 16% of resected pancreatic cystic tumors [31] and are most common in the body or tail of the pancreas, [6],[8] but can involve the entire organ. [31] Up to 90% of patients with von Hippel-Lindau syndrome have been reported to develop SCN. [6]
Diagnosis
SCNs are usually <5 cm in diameter (median size of 25-30 mm), [32] but can be as large as 25 cm [5] and appear macroscopically as small cysts with a stellate scar. [32] The cells are lined by a glycogen-rich cuboidal epithelium, [6],[8],[9] have clear cytoplasm with well-delineated borders, do not produce mucin, [32] and do not communicate with the PD. [6] Depending on their degree of dysplasia, they can be classified as either SCA or serous cystadenocarcinoma (SCAC). [6]
Serous cystadenomas can be divided into polycystic, honeycomb, and oligocystic/macrocystic forms. The polycystic form is most common (70%), and is represented by a collection (usually >6) of small cysts, generally <2 cm in size. [5],[33] On CT, a central fibrous scar with calcification can be seen in up to 30% of these lesions and is pathognomonic for SCNs. [5],[6],[34] Microcysts can appear solid or show macrocavity, which can lead to confusion of these tumors with MCN. MCN, however, are usually unilocular or multilocular and have a small number of discrete compartments. [9] The honeycomb pattern is seen in 20% of patients and has multiple subcentimeter cysts that appear as solid masses on CT and maintain high signal intensity on T2-weighted MRI. [33] The oligocystic (macrocystic) pattern is the least common (<10%) and can be difficult to distinguish from MCN based on MRI or CT. [6],[32],[34] The presence of 3 or more of the following criteria on CT scan has been shown to have a 100% specificity in differentiating macrocystic SCA from MCN and PC: (1) location within the pancreatic head, (2) lobulated contour of the cyst wall, (3) cyst wall thickness of <2 mm, and (4) absence of cyst wall enhancement. [35] On EUS, SCNs will appear as small, anechoic cystic lesions with thin septations, [6] may have calcification of central septae, [34] and have a honeycomb appearance with several <3 mm cysts. [36] Fluid from SCAs typically has a low level of CEA, usually <5 ng/mL (specificity 95%) [Table 1]. [31]
Management
Malignant transformation of a SCA (into SCAC) is extremely rare, with approximately 30 reported cases in the literature as of 2014. [37] Thus, current guidelines only recommend surgical resection for size >4 cm (although some surgeons may not operate just for size >4 cm in the absence of symptoms or suspicion for malignancy), presence of symptoms, and uncertainty about the true nature of the cystic lesion. [6],[34],[38] Patients with the oligocystic/macrocystic variety and/or a history of nonpancreatic malignancies are more likely to have significant tumor growth requiring a resection in the future. [38] Follow-up imaging for asymptomatic, nonresected patients is suggested within 3-6 months. [37],[39] There is debate regarding surveillance imaging beyond this point. [37] Although consensus guidelines have suggested follow-up for these patients on a semi-annual or annual basis, [38],[40] some studies support follow-up after 2 years. [38] In patients who have had surgical resection, postoperative surveillance is unnecessary [40] unless histology showed SCAC. [37]
Cystic Pancreatic Endocrine Neoplasm
Cystic pancreatic endocrine neoplasms account for approximately 8% of resected PCN [31],[41] and 10-15% of resected pancreatic neuroendocrine tumors. [31] Most are found incidentally and are nonfunctioning. They occur equally in men and women, are usually diagnosed at 60-70 years of age, [31] and are more frequently located in the body and tail of the pancreas. [8] They are more common in patients with multiple endocrine neoplasia type I (MEN-1), [31],[42] with one study finding MEN-I to be 3.5 times more likely in CPEN than in solid tumors. [42]
Diagnosis
On imaging, the lesions may have a hypervascular rim (77%) [31],[43] and may contain septations or a solid component. [31],[44] On ultrasound, there will be a well-circumscribed, uniform wall around areas of cystic degeneration and a less uniform wall around areas of necrosis. [45] On MRI, the peripheral rim will be moderately hyperintense on fat-saturated T2-weighted images, and hypointense on fat-saturated T1-weighted imaging. [45]
If characteristic imaging findings are not present or if a preoperative diagnosis is necessary, EUS with FNA may be useful. [44] Fluid aspiration will reveal low levels of CEA. [7],[31] Cytology will reveal minimal cytoplasm and monomorphic nuclei with “salt-and-pepper” chromatin [Table 1]. [8],[9] Immunohistochemical (IHC) staining for chromogranin and synaptophysin is frequently seen, [7],[44] and in one study, cytologic diagnosis was possible in approximately 80% of cases. [44] Cyst fluid studies of amylase or CA 19-9 have not proven to be helpful. [44]
Management
Similar to other endocrine pancreatic tumors, malignancy may be difficult to determine, even with biopsy or gross examination during surgery. [31] Although these lesions are indolent in nature, they are considered premalignant, and surgery is recommended for appropriate candidates, especially with lesions >2 cm in size. [8] Some authors recommend surgical resection for all patients, with overall excellent prognosis. [31],[44] In one study, the 1-year and 5-year survival after resection were 97% and 87%, respectively. [42]
Mucinous Cystic Neoplasms
Although MCN can be benign, they are most commonly premalignant or malignant, [1] and represent approximately 25% of resected PCN. [31] They are more common in women (>95%) [31],[37] and are usually located in the distal pancreas (>95%), [31] with a peak incidence in the fifth decade. [6],[37] They usually grow to a size of 8-10 cm, but can be as large as 25 cm. [5],[46] The World Health Organization has classified MCN into three stages: Benign (adenomatous), low-grade malignant (borderline), and malignant (carcinoma in situ and invasive). [9] In one study of 168 patients, 72% had adenomas, 10.5% borderline neoplasms, 5.5% carcinoma in situ, and 12% invasive carcinoma. In this study, factors associated with malignancy included presence of nodules and a diameter ≥60 mm. [47]
Diagnosis
Histologically, MCN are lined by mucin-secreting columnar epithelial cells. [6],[48] A dense, ovarian-like stroma is a finding unique to MCN; [6],[8],[9],[31] it was seen in 76% of cases in one series, [49] and some authors consider it a prerequisite for diagnosis of MCN. [6],[50] MCN often resemble IPMN; however, unlike IPMN, they have an ovarian stroma and often lack communication with the pancreatic ductal system. [6],[8],[9],[51] Additionally, unlike BD-IPMN, they are always single lesions. [31],[47]
On CT imaging, they appear as large cysts with thin septae that are best seen with intravenous contrast. [6] They may have lamellated calcifications peripherally, whereas SCN often have central, stellate calcifications. [6] In 15% of cases, peripheral eggshell calcifications may be found on CT, [9],[46] and this finding indicates an increased likelihood of invasive cystadenocarcinoma. [5] Other imaging findings that are associated with invasive carcinoma include papillary invaginations, an eccentrically located mass in a cystic area, large size (usually >2 or 3 cm), a recognizable pericystic mass/reaction, wall or septal/papillary enhancement, local invasion of adjacent vascular structures, associated metastatic lesions, extrahepatic biliary obstruction, and/or splenic venous occlusion. [5],[46],[52] On MRI, MCN have high signal intensity on T2-weighted images. [6] In one series, all malignant MCN either had nodules or were >4 cm, with a malignancy rate of 17.5%. [31],[47]
On EUS, the cysts appear as thin-walled, septated fluid-filled cavities. A recent meta-analysis of 376 patients who underwent EUS-FNA cytology and histopathological diagnosis showed a sensitivity and specificity of 63% and 88%, respectively, in diagnosing pancreatic MCN. [1] Cyst fluid studies will have high CEA due to secretion of mucin, but fluid studies cannot necessarily be used to distinguish them from IPMN. [6] Additional fluid characteristics include high CEA and low amylase levels [Table 1]. [45]
Because MCN usually do not communicate with the PD, endoscopic retrograde cholangiopancreatography is rarely performed, [6] but can be used to distinguish MCN from BD-IPMN. [46] Another distinguishing factor is that while MCN are more common among middle-aged women and are more often located in the pancreatic tail, side-branch IPMN are more common in older men and are more frequently located in the proximal pancreas. [15] EUS findings associated with malignant MCN include size >4 cm, cyst wall irregularity and thickening, septal thickening, intracystic solid regions, presence of wall calcification, PD dilation, presence of collateral vessels, and the presence of a frank mass or mural nodules. [46]
Management
Observation may be considered in elderly patients, [47],[49],[53] especially those with lesions <3 cm and no intramural nodules. [47],[49] However, because the natural history of MCN is still unknown and most patients are relatively young (and thus have a risk of progression to invasive MCN), surgical resection is recommended for all patients who are surgically fit and have no contraindications. [32],[47],[53] Because most MCN are located in the body or tail of the pancreas, distal pancreatectomy is often the procedure of choice, and has been safely performed at high-volume centers. [47],[53] Studies have reported a 5-year survival of 94.7-100% in patients with noninvasive MCN and 57-62.5% in those with invasive MCN. [47],[48] In patients with invasive carcinoma, disease recurrence ranges from 37% to 83% at 5 years. [37],[47]
After surgical resection, patients without tissue invasion probably do not need follow-up imaging. [46],[53] However, those with invasion are recommended to get repeat CT or MRI every 6 months to assess for local recurrence and distant metastases. [15],[46]
Intraductal Papillary Mucinous Neoplasm
IPMN are cystic lesions of the pancreas lined by intraductal dysplastic epithelium, which secrete excessive mucin, causing cystic dilation of the PDs. IPMNs are characterized by ductal involvement, which distinguishes them from MCNs. IPMNs can be divided into three types: Main-duct IPMN (MD-IPMN), BD-IPMN, and mixed IPMN. MD involvement is defined by segmental or diffuse dilation of the main PD to >5 mm in the absence of obstruction. This definition reflects the changes in the Fukuoka Guidelines from 2012 (International consensus guidelines for the management of IPMN and MCN of the pancreas), where PD dilation to >5 mm (previously >10 mm) can be used to characterize MD-IPMN, as this increases the sensitivity and maintains the specificity of radiologic diagnosis. [50],[53],[54],[55],[56],[57],[58],[59],[60] BD-IPMNs are cystic lesions which connect to the MD, and are not PC. Mixed IPMN show features of both MD-IPMN and BD-IPMN.
IPMN usually occur in the seventh decade of life and occur more frequently in males, with the highest male to female ratio of 3:1 seen in the Asian population. [31] IPMNs can be present throughout the pancreas but most often are confined to the pancreatic head (>50% of the time). [60] BD-IPMNs can be isolated lesions or larger collections of pancreatic cysts; 21-41% of those with BD-IPMNs have multi-focal disease, with >2 cysts of various sizes throughout the pancreas. [31],[53],[57],[61] Common symptoms of IPMN at presentation include abdominal pain, weight loss, jaundice, and acute pancreatitis, which are more frequently seen with MD-IPMN/mixed IPMN than BD-IPMN. [60],[62] BD-IPMN is usually asymptomatic and incidentally found, but sometimes can cause pancreatitis symptoms.
With regard to risk factors for IPMN, a recent study showed that a history of diabetes (especially with prior insulin use), chronic pancreatitis, and family history of pancreatic adenocarcinoma may increase risk of IPMN development. [63]
Overall, BD-IPMNs are more indolent, with mean frequency of malignancy and invasive carcinoma around 25% and 18%, respectively, compared with 61% and 43% in MD-IPMN, respectively. [53],[56],[57],[58],[59],[60],[61],[64],[65],[66],[67],[68],[69],[70],[71],[72],[73],[74],[75],[76]
It is thought that the histologic subtype of the papillary component of IPMNs may affect its malignant potential. [77],[78],[79] Gastric-type histology is seen more commonly in BD-IPMNs and is associated with more benign behavior; however, if tubular adenocarcinoma arises from gastric-type mucosa, it is associated with a very poor prognosis. Intestinal-type histology is found more frequently in MD-IPMN and is associated with intermediate to high risk of dysplasia; it is therefore thought to cause more aggressive disease than gastric-type histology. [80],[81],[82] However, colloid carcinoma, which develops in the setting of intestinal-type IPMN, has a better prognosis than tubular adenocarcinoma arising from gastric-type mucosa. Of all the histologic subtypes, pancreaticobiliary histology is most likely to be seen in invasive cancer arising from IPMN. However, there is still debate if histologic subtype actually affects disease-specific survival. [78],[79],[81]
Diagnosis and Management
Imaging studies for further work-up of possible MD-IPMN or BD-IPMN include gadolinium-enhanced MRI with magnetic resonance cholangiopancreatography (MRCP) or CT pancreatic protocol, although recent studies have shown that a dedicated MRI is preferred secondary to superior contrast resolution, which aids in delineating septae, nodules, and duct communication. [83] Dedicated pancreatic imaging should be performed when standard imaging notes presence of a pancreatic cystic lesion >1 cm. Detection of a hypo-attenuating region by CT in a case of suspected IPMN may indicate a malignant lesion. [84]
To determine further management of suspected IPMNs after initial evaluation with CT or MRI (i.e., surgical resection, further evaluation with EUS, or surveillance), the 2012 Fukuoka Guidelines should be utilized. Previous Sendai Consensus Guidelines of 2006 recommended surgical resection of suspected MD-IPMN when PD diameter was >10 mm. These guidelines also recommended resection of suspected BD-IPMN with cyst size >3 cm or cyst size <3 cm and presence of mural nodules, dilation of the main PD >6 mm, symptoms attributable to the cyst, and positive cytology. [50] These guidelines were revised and expanded in 2012 (and now called Fukuoka Guidelines), with characterization of certain IPMN cyst characteristics as “high-risk stigmata” or “worrisome features” to aid in management of IPMNs, particularly BD-IPMNs. [53] Using the Fukuoka Guidelines, “high-risk stigmata” include presence of pancreatic head mass (with resulting obstructive jaundice), enhancing solid component, and main PD >10 mm. Given the increased risk of malignant IPMN, these lesions should be surgically resected. “Worrisome features” include cyst size of >3 cm, main PD size of 5-9 mm, thickened enhanced cyst walls, presence of nonenhancing mural nodules, lymphadenopathy, and distal pancreatic atrophy with abrupt change in caliber of the PD. [55],[57],[58],[61],[66],[71],[76] Suspected IPMNs with cyst size >3 cm without “worrisome features” or cyst size <3 cm with other “worrisome features” warrant further investigation with EUS to evaluate for concerning features such as definite mural nodule and evidence of MD involvement. In addition, FNA with cytology should be performed during EUS to rule-out malignancy. According to one meta-analysis, EUS-FNA accurately diagnosed IPMNs 72% of the time. [1] Furthermore, intraductal ultrasound appears to be useful in differentiating invasive IPMNs from benign lesions but is not routinely used. [85] A recent study by Lee et al. showed that an EUS scoring system using pancreatic cyst size, height of mural nodules, MD dilation, septal thickening, and patulous orifice was more accurate at predicting malignancy than the Sendai Consensus Guidelines. [86]
It should be noted that the finding of “high-grade atypical epithelial cells” on FNA can also be a sensitive predictor of malignancy and in one study, was considered a more accurate predictor of malignancy than “positive” cytology. [87] In general, IPMNs will have clear viscous fluid (positive “string sign”) and elevated CEA >192 (reflective of a mucinous neoplasm, not malignancy) in the cyst fluid analysis; in addition, extracellular mucin can be noted. [19] These features are seen with both MCN and IPMNs.
Cyst fluid markers that may predict malignancy are being evaluated. It appears that GNAS mutations may predict progression to invasive cancer in IPMNs. [28] A recent study by Sadot et al. found that higher levels of tumor-associated neutrophils as well as cyst fluid inflammatory proteins (interferon-gamma, tissue inhibitor of metalloproteinase-1, macrophage inhibitory factor, tumour necrosis factor-alpha, and matrix metalloproteinase-9) were associated with higher grades of dysplasia. [88]
There have also been several studies evaluating the use of pancreatic juice cytology to detect malignancy. One study by Ohtsuka et al. showed good sensitivity and specificity for detection of malignancy, especially in suspected IPMNs with “worrisome features.” [89] Another study by Hirono et al. showed that pancreatic juice CEA level >30 was an independent predictor for malignancy for BD-IPMN. [90]
A recent study evaluating peroral pancreatoscopy (SpyGlass) for assessment of IPMN with MD involvement revealed poor sensitivity but 100% specificity of direct visualization biopsies for detecting malignancies; however, irrigation cytology had 100% sensitivity and specificity for detecting malignancy. [91] This may be a potential tool for further characterizing suspected IPMNs.
There have been many studies evaluating the utility of the Sendai Consensus Guidelines and Fukuoka Guidelines for management of IPMN, often with incongruous results. A recent meta-analysis by Goh et al. showed that the Sendai Consensus Guidelines had a low PPV (11-52%) but a high NPV (90-100%) for predicting malignancy in BD-IPMN. [92] Another meta-analysis evaluating the 2006 Sendai Consensus Guidelines showed that cyst features proposed by the guidelines for resection of IPMN were highly associated with malignancy, with cyst size >3 cm associated most strongly with malignant IPMN. This conclusion differs somewhat from the findings of a meta-analysis by Kim et al. which showed that the presence of mural nodules in a suspected BD-IPMN is highly suspicious for malignancy, whereas cyst size >3 cm, MPD dilation, and thick wall/septum are weaker indicators of malignancy. [93],[94] Other studies have shown that a fair number of “Sendai negative” IPMNs can harbor malignancy and that these lesions can be undertreated if the guidelines are followed too closely. [68],[95],[96],[97] Another recent study showed that the “high-risk” features of the Fukuoka Guidelines correlated significantly with the grade of malignancy of BD-IPMNs, but the “worrisome features” did not correlate with the malignant grade of BD-IPMNs. [98] Other proposed high-risk factors to aid in identification of malignant BD-IPMNs include rapidly increasing cyst size, mural nodule >10 mm in height, and “high-grade atypical epithelial cells” in place of “positive” cytology, as was previously discussed. [87],[99]
Given that radiologic studies cannot always predict which IPMNs will be malignant, many studies have been done to identify markers that can distinguish between high-grade and low-grade lesions. The Notch signaling pathway has been associated with malignant transformation of IPMN. Ishikawa et al. showed that Notch pathway epithelial-mesenchymal transition transcription factors Twist and BMI1 expression were significantly higher in resected IPMNs with high-grade dysplasia and invasive carcinoma than in those with low-grade dysplasia. [100] Ikemoto et al. showed that disease-free survival was significantly worse in Notch 1 high-expression IPMNs, and that Notch 2 family expressions were higher in intraductal papillary mucinous carcinoma than in intraductal papillary mucinous adenoma. [101] Further studies are needed to further elucidate which signaling pathways are involved with malignant transformation of IPMN and to discover serum, cyst fluid, and tumor markers that can predict which IPMNs are malignant.
If concerning features are noted on EUS, surgical resection of the pancreatic lesion should be performed. On the other hand, if concerning features are absent, follow-up surveillance is determined by cyst size. However, factors such as age, operative risk, location of IPMN, and comorbidities should also be considered when determining management of IPMN. [31],[102] Importantly, BD-IPMNs occur mostly in the elderly population and are less likely to be malignant or invasive compared with MD-IPMNs. Based on Fukuoka guidelines, BD-IPMNs <2 cm in size without “worrisome features” on MRI/MRCP or EUS can be monitored with surveillance imaging. BD-IPMN <1 cm in size should be followed-up with CT/MRI in 2-3 years, and BD-IPMNs that are 1-2 cm should be followed with yearly imaging for 2 years. BD-IPMNs that are 2-3 cm should be followed by EUS in 3-6 months, with consideration for surgical resection in younger (<65 years old) healthy patients given lifetime cumulative malignancy risk. BD-IPMNs >3 cm should be surgically resected in young, healthy patients or be followed with EUS or MRI every 3-6 months initially, with lengthened intervals thereafter. [53]
On the other hand, MD-IPMNs are more likely to harbor malignancy and have low 5-year survival rates, so surgically fit patients should undergo resection. However, it is unclear if those with main PD dilation to 5-9 mm (“worrisome features”) need immediate surgery. Preoperative cytology and serum CA 19-9 levels may also be helpful in predicting malignant MD-IPMNs and need for surgery. [103]
The goal of surgical resection for IPMNs is complete resection with negative margins. If resection margins are positive for dysplasia (particularly high-grade dysplasia), further pancreatic resection should be performed until resection margins are negative. Standard resection surgeries for invasive IPMNs include: pancreatoduodenectomy, distal pancreatectomy, or total pancreatectomy (depending on the site and extent of disease) with lymph node dissection; more extensive pancreatic surgery can lead to brittle diabetes and exocrine insufficiency. Therefore, those BD-IPMNs presumed not to be invasive (i.e., those with mural nodules <5 mm in height, MD dilation <10 mm, or absence of solid mass) can be treated with parenchyma-sparing resections, including central pancreatectomy, enucleation, or uncinatectomy; however, these procedures may be associated with higher risk of mucin leakage with development of pseudomyxoma peritonei, pancreatic fistula formation, and residual disease. These parenchyma-sparing procedures have been shown to preserve pancreatic endocrine/exocrine function and can have good long-term outcomes (10-year progression-free survival of 76%, with only 4% need for reoperation of recurrent lesions in one study). [104] Multifocal BD-IPMN may require total pancreatectomy, although segmental resection is an option for multifocal disease restricted to a particular region of the pancreas or multifocal disease with the highest risk lesions confined to a particular pancreatic region.
With regard to surgical management of MD-IPMN, the segmental ectatic type or diffuse type with focal lesions can be treated with proximal or distal pancreatectomy, depending on the location of the lesion. On the other hand, MD-IPMN with diffuse dilation should be treated with right pancreatectomy, as it is easier to extend the resection bed to ensure negative margins.
For those who are not surgical candidates or elect to forego surgery but have “high risk stigmata,” follow-up MRI/MRCP should be done every 3-6 months. One study evaluating “Sendai positive” IPMNs which were not resected showed that that the median overall survival in this cohort was 52 months, with 5-year overall survival of 35% and 5-year disease-specific survival of 48%; only MD involvement was associated with worse disease-specific survival. [105]
After surgical resection, those with known remaining IPMN should be followed with MRI/MRCP every 3-9 months. For those with negative margins after surgical resection (i.e., normal pancreatic tissue or nondysplastic changes at the resection margin) without remaining lesions, surveillance evaluations can be done 2 and 5 years after resection. On the other hand, for those with noninvasive IPMN after surgery (i.e. remaining low, moderate, or high-grade dysplasia), surveillance MRI twice per year should be done.
IPMN recurrence rate in the first 5 years after surgical resection is between 0% and 20%. In general, noninvasive disease has a 5-year disease-specific survival approaching 100%, while invasive disease has a 5-year survival most commonly reported around 60% (range: 31-65%). [60],[67],[69],[76],[106] For noninvasive resected IPMNs, family history of pancreatic cancer may be a risk factor for development of new or progressive IPMN. According to one study, the 5-year overall survival rate for MD-IPMN post-resection was around 70% with disease-specific survival rate of 83%. Size/type of invasive component, lymph node positivity, and positive resection margin were the most important predictors for survival and recurrence. [107] Another study showed a post-resection IPMN recurrence rate of 10.7% (median follow-up of 44 months) with overall 5-year disease-free survival of 78.9%; pathologic grade of dysplasia was the most important predictor of recurrence and was inversely related to disease-free survival. [108]
Finally, it should be noted that there is a 20-30% occurrence of extrapancreatic malignancy in patients with IPMNs, including GI, skin, breast, renal cell, thyroid, and prostate malignancies. [109] However, at this time, there are no guidelines regarding special screening for extrapancreatic malignancies outside of standard screening for patients with IPMN.
The present guidelines include recent information and recommendations based on our current understanding, and highlight issues that remain controversial and areas where further research is required. [53]
Solid Pseudopapillary Neoplasms
SPNs are uncommon cystic lesions of the pancreas, accounting for <4% of resected pancreatic cystic lesions. They have a gender predilection for females (>80%) and occur in the third and fourth decades of life. [110],[111],[112] SPNs are genetically characterized by activation of beta-catenin and its target genes in the WNT signaling pathway. [112],[113] SPNs can occur throughout the pancreas but usually occur in the pancreatic body or tail, and usually present with nonspecific symptoms such as abdominal discomfort, increased abdominal girth, and poor appetite and nausea from tumor compression of adjacent organs. They usually are discovered incidentally now with the increased use of radiologic assessments. [31],[114],[115] Presentation with pancreatitis, jaundice, weight loss, or palpable mass is rare. SPNs appear as large, well-demarcated, solitary, mixed solid and cystic heterogeneous masses. It is thought that these tumors begin as solid masses with poorly supported small vessels; therefore the cells farthest from the vessels undergo swelling and degenerative change, while cells adjacent to the vessels remain intact, resulting in a pseudopapillary pattern and cystic spaces. [116]
Diagnosis
Computed tomography evaluation shows no enhancement of the cystic portions, but slight enhancement of the solid portions in the arterial phase and marked enhancement in the portal venous phase; peripheral arterial enhancement and central calcification can also be seen. [110],[117] Accuracy of EUS with FNA for diagnosis of SPNs is around 69%. [118] Gross appearance of the tumor reveals a fibrous pseudocapsule, variegated appearance, and variable combinations of solid hemorrhagic and necrotic cystic areas. [119] Histologic appearance shows discohesive polygonal cells that surround delicate blood vessels and form a solid mass with frequent cystic degeneration and intracystic hemorrhage. [115],[120] IHC studies show positivity for vimentin, CD10, CD56, alpha-1-antitrypsin, and usually Neuron-specific enolase; immunoreactivity for beta-catenin is almost always found. [115]
Management
Although SPNs usually have an indolent course, given the malignant potential of these lesions, patients are usually treated with surgical resection. Surgical management depends on the location of the SPN and includes distal pancreatectomy, central pancreatectomy, local resection, enucleation, and pancreaticoduodenectomy. There is debate about the optimal extent and type of surgery for SPN. [120],[121] The goal of resection is to obtain negative margins. Most patients have localized disease, but 10-15% have metastatic disease. [120],[122],[123] Common metastatic sites include the liver, IVC wall, and spleen. [114] Despite locally aggressive features and even presence of metastatic disease, SPNs have a favorable prognosis. Surgery is the treatment of choice, even for treatment of metastatic lesions and locally recurrent tumors. [115],[116],[124],[125] There is a <2% mortality rate associated with surgical resection, and the 5-year survival rate is around 95% after surgical resection. [118] There is limited data regarding adjuvant chemotherapy or radiotherapy. The mean time to tumor recurrence is 4 years, suggesting that patients should undergo postoperative surveillance for at least 5 years, although no definitive surveillance guidelines exist. [118] There is some evidence to suggest that male patients, older patients, those with SPNs with atypical histopathology (tumor > 5 cm, diffuse growth, cellular/nuclear atypia, high mitotic activity, necrosis, or extrapancreatic invasion/metastasis), and those with incomplete resection may have increased mortality and increased risk of recurrence; these patients should be followed more closely. [121]
Conclusion
Due to improvements in endoscopic and cross-sectional imaging modalities, we are now able to more quickly and accurately diagnosis pancreatic cystic lesions. These tools are essential to distinguishing benign from malignant lesions, while also determining the potential for malignant transformation. A multidisciplinary approach involving gastroenterologists, surgeons, and radiologists is needed to ensure the most appropriate management for each patient. While new guidelines offer recommendations for identifying higher-risk lesions, each patient must be assessed on a case-by-case basis, and further research is required in areas that remain controversial.
References
| 1. |
Thosani N, Thosani S, Qiao W, Fleming JB, Bhutani MS, Guha S. Role of EUS-FNA-based cytology in the diagnosis of mucinous pancreatic cystic lesions: A systematic review and meta-analysis. Dig Dis Sci 2010;55:2756-66.
 |
| 2. |
Moparty B, Logroño R, Nealon WH, Waxman I, Raju GS, Pasricha PJ, et al. The role of endoscopic ultrasound and endoscopic ultrasound-guided fine-needle aspiration in distinguishing pancreatic cystic lesions. Diagn Cytopathol 2007;35:18-25.
|
| 3. |
Warshaw AL, Compton CC, Lewandrowski K, Cardenosa G, Mueller PR. Cystic tumors of the pancreas. New clinical, radiologic, and pathologic observations in 67 patients. Ann Surg 1990;212:432-43.
|
| 4. |
Sohn TA, Yeo CJ, Cameron JL, Iacobuzio-Donahue CA, Hruban RH, Lillemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: An increasingly recognized clinicopathologic entity. Ann Surg 2001;234:313-21.
|
| 5. |
Sakorafas GH, Sarr MG. Cystic neoplasms of the pancreas; what a clinician should know. Cancer Treat Rev 2005;31:507-35.
|
| 6. |
Yoon WJ, Brugge WR. Pancreatic cystic neoplasms: Diagnosis and management. Gastroenterol Clin North Am 2012;41:103-18.
|
| 7. |
Enestvedt BK, Ahmad N. To cease or ′de-cyst′? The evaluation and management of pancreatic cystic lesions. Curr Gastroenterol Rep 2013;15:348.
|
| 8. |
Clores MJ, Thosani A, Buscaglia JM. Multidisciplinary diagnostic and therapeutic approaches to pancreatic cystic lesions. J Multidiscip Healthc 2014;7:81-91.
|
| 9. |
Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218-26.
|
| 10. |
Bhutani MS, Gupta V, Guha S, Gheonea DI, Saftoiu A. Pancreatic cyst fluid analysis – A review. J Gastrointestin Liver Dis 2011;20:175-80.
|
| 11. |
Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: A report of the cooperative pancreatic cyst study. Gastroenterology 2004;126:1330-6.
|
| 12. |
Tomimaru Y, Takeda Y, Tatsumi M, Kim T, Kobayashi S, Marubashi S, et al. Utility of 2-[18F] fluoro-2-deoxy-D-glucose positron emission tomography in differential diagnosis of benign and malignant intraductal papillary-mucinous neoplasm of the pancreas. Oncol Rep 2010;24:613-20.
|
| 13. |
Sperti C, Bissoli S, Pasquali C, Frison L, Liessi G, Chierichetti F, et al. 18-fluorodeoxyglucose positron emission tomography enhances computed tomography diagnosis of malignant intraductal papillary mucinous neoplasms of the pancreas. Ann Surg 2007;246:932-7.
|
| 14. |
Hong HS, Yun M, Cho A, Choi JY, Kim MJ, Kim KW, et al. The utility of F-18 FDG PET/CT in the evaluation of pancreatic intraductal papillary mucinous neoplasm. Clin Nucl Med 2010;35:776-9.
|
| 15. |
Sahani DV, Kambadakone A, Macari M, Takahashi N, Chari S, Fernandez-del Castillo C. Diagnosis and management of cystic pancreatic lesions. AJR Am J Roentgenol 2013;200:343-54.
|
| 16. |
Brandwein SL, Farrell JJ, Centeno BA, Brugge WR. Detection and tumor staging of malignancy in cystic, intraductal, and solid tumors of the pancreas by EUS. Gastrointest Endosc 2001;53:722-7.
|
| 17. |
Sedlack R, Affi A, Vazquez-Sequeiros E, Norton ID, Clain JE, Wiersema MJ. Utility of EUS in the evaluation of cystic pancreatic lesions. Gastrointest Endosc 2002;56:543-7.
|
| 18. |
Cizginer S, Turner BG, Bilge AR, Karaca C, Pitman MB, Brugge WR. Cyst fluid carcinoembryonic antigen is an accurate diagnostic marker of pancreatic mucinous cysts. Pancreas 2011;40:1024-8.
|
| 19. |
Rockacy M, Khalid A. Update on pancreatic cyst fluid analysis. Ann Gastroenterol 2013;26:122-7.
|
| 20. |
Snozek CL, Mascarenhas RC, O′Kane DJ. Use of cyst fluid CEA, CA19-9, and amylase for evaluation of pancreatic lesions. Clin Biochem 2009;42:1585-8.
|
| 21. |
van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: A pooled analysis. Gastrointest Endosc 2005;62:383-9.
|
| 22. |
Hammel P, Voitot H, Vilgrain V, Lévy P, Ruszniewski P, Bernades P. Diagnostic value of CA 72-4 and carcinoembryonic antigen determination in the fluid of pancreatic cystic lesions. Eur J Gastroenterol Hepatol 1998;10:345-8.
|
| 23. |
Pais SA, Attasaranya S, Leblanc JK, Sherman S, Schmidt CM, DeWitt J. Role of endoscopic ultrasound in the diagnosis of intraductal papillary mucinous neoplasms: Correlation with surgical histopathology. Clin Gastroenterol Hepatol 2007;5:489-95.
|
| 24. |
Al-Rashdan A, Schmidt CM, Al-Haddad M, McHenry L, Leblanc JK, Sherman S, et al. Fluid analysis prior to surgical resection of suspected mucinous pancreatic cysts. A single centre experience. J Gastrointest Oncol 2011;2:208-14.
|
| 25. |
Frossard JL, Amouyal P, Amouyal G, Palazzo L, Amaris J, Soldan M, et al. Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions. Am J Gastroenterol 2003;98:1516-24.
|
| 26. |
Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N, Ahmad N, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: A report of the PANDA study. Gastrointest Endosc 2009;69:1095-102.
|
| 27. |
Sawhney MS, Devarajan S, O′Farrel P, Cury MS, Kundu R, Vollmer CM, et al. Comparison of carcinoembryonic antigen and molecular analysis in pancreatic cyst fluid. Gastrointest Endosc 2009;69:1106-10.
|
| 28. |
Wu J, Matthaei H, Maitra A, Dal Molin M, Wood LD, Eshleman JR, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci Transl Med 2011;3:92ra66.
|
| 29. |
Konda VJ, Meining A, Jamil LH, Giovannini M, Hwang JH, Wallace MB, et al. A pilot study of in vivo identification of pancreatic cystic neoplasms with needle-based confocal laser endomicroscopy under endosonographic guidance. Endoscopy 2013;45:1006-13.
|
| 30. |
Napoléon B, Lemaistre AI, Pujol B, Caillol F, Lucidarme D, Bourdariat R, et al. A novel approach to the diagnosis of pancreatic serous cystadenoma: Needle-based confocal laser endomicroscopy. Endoscopy 2015;47:26-32.
|
| 31. |
Farrell JJ, Fernández-del Castillo C. Pancreatic cystic neoplasms: Management and unanswered questions. Gastroenterology 2013;144:1303-15.
|
| 32. |
Atiq M, Suzuki R, Khan AS, Krishna SG, Ridgway TM, Guha S, et al. Clinical decision making in the management of pancreatic cystic neoplasms. Expert Rev Gastroenterol Hepatol 2013;7:353-60.
|
| 33. |
Sarr MG, Murr M, Smyrk TC, Yeo CJ, Fernandez-del-Castillo C, Hawes RH, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastrointest Surg 2003;7:417-28.
|
| 34. |
Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited. Part I: Serous cystic neoplasms. Surg Oncol 2011;20:e84-92.
|
| 35. |
Cohen-Scali F, Vilgrain V, Brancatelli G, Hammel P, Vullierme MP, Sauvanet A, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: Initial observations. Radiology 2003;228:727-33.
|
| 36. |
Zaheer A, Pokharel SS, Wolfgang C, Fishman EK, Horton KM. Incidentally detected cystic lesions of the pancreas on CT: Review of literature and management suggestions. Abdom Imaging 2013;38:331-41.
|
| 37. |
Robinson SM, Scott J, Oppong KW, White SA. What to do for the incidental pancreatic cystic lesion? Surg Oncol 2014;23:117-25.
|
| 38. |
Malleo G, Bassi C, Rossini R, Manfredi R, Butturini G, Massignani M, et al. Growth pattern of serous cystic neoplasms of the pancreas: Observational study with long-term magnetic resonance surveillance and recommendations for treatment. Gut 2012;61:746-51.
|
| 39. |
Del Chiaro M, Verbeke C, Salvia R, Klöppel G, Werner J, McKay C, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013;45:703-11.
|
| 40. |
Katz MH, Mortenson MM, Wang H, Hwang R, Tamm EP, Staerkel G, et al. Diagnosis and management of cystic neoplasms of the pancreas: An evidence-based approach. J Am Coll Surg 2008;207:106-20.
|
| 41. |
Valsangkar NP, Morales-Oyarvide V, Thayer SP, Ferrone CR, Wargo JA, Warshaw AL, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012;152:S4-12.
|
| 42. |
Bordeianou L, Vagefi PA, Sahani D, Deshpande V, Rakhlin E, Warshaw AL, et al. Cystic pancreatic endocrine neoplasms: A distinct tumor type? J Am Coll Surg 2008;206:1154-8.
|
| 43. |
Ligneau B, Lombard-Bohas C, Partensky C, Valette PJ, Calender A, Dumortier J, et al. Cystic endocrine tumors of the pancreas: Clinical, radiologic, and histopathologic features in 13 cases. Am J Surg Pathol 2001;25:752-60.
|
| 44. |
Gaujoux S, Tang L, Klimstra D, Gonen M, Brennan MF, D′Angelica M, et al. The outcome of resected cystic pancreatic endocrine neoplasms: A case-matched analysis. Surgery 2012;151:518-25.
|
| 45. |
Dewhurst CE, Mortele KJ. Cystic tumors of the pancreas: Imaging and management. Radiol Clin North Am 2012;50:467-86.
|
| 46. |
Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited: Part II. Mucinous cystic neoplasms. Surg Oncol 2011;20:e93-101.
|
| 47. |
Crippa S, Salvia R, Warshaw AL, Domínguez I, Bassi C, Falconi M, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: Lessons from 163 resected patients. Ann Surg 2008;247:571-9.
|
| 48. |
Yamao K, Yanagisawa A, Takahashi K, Kimura W, Doi R, Fukushima N, et al. Clinicopathological features and prognosis of mucinous cystic neoplasm with ovarian-type stroma: A multi-institutional study of the Japan pancreas society. Pancreas 2011;40:67-71.
|
| 49. |
Reddy RP, Smyrk TC, Zapiach M, Levy MJ, Pearson RK, Clain JE, et al. Pancreatic mucinous cystic neoplasm defined by ovarian stroma: Demographics, clinical features, and prevalence of cancer. Clin Gastroenterol Hepatol 2004;2:1026-31.
|
| 50. |
Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006;6:17-32.
|
| 51. |
Zamboni G, Scarpa A, Bogina G, Iacono C, Bassi C, Talamini G, et al. Mucinous cystic tumors of the pancreas: Clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol 1999;23:410-22.
|
| 52. |
Ng DZ, Goh BK, Tham EH, Young SM, Ooi LL. Cystic neoplasms of the pancreas: Current diagnostic modalities and management. Ann Acad Med Singapore 2009;38:251-9.
|
| 53. |
Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183-97.
|
| 54. |
Kawamoto S, Lawler LP, Horton KM, Eng J, Hruban RH, Fishman EK. MDCT of intraductal papillary mucinous neoplasm of the pancreas: Evaluation of features predictive of invasive carcinoma. AJR Am J Roentgenol 2006;186:687-95.
|
| 55. |
Hwang DW, Jang JY, Lee SE, Lim CS, Lee KU, Kim SW. Clinicopathologic analysis of surgically proven intraductal papillary mucinous neoplasms of the pancreas in SNUH: A 15-year experience at a single academic institution. Langenbecks Arch Surg 2012;397:93-102.
|
| 56. |
Serikawa M, Sasaki T, Fujimoto Y, Kuwahara K, Chayama K. Management of intraductal papillary-mucinous neoplasm of the pancreas: Treatment strategy based on morphologic classification. J Clin Gastroenterol 2006;40:856-62.
|
| 57. |
Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, et al. Intraductal papillary mucinous neoplasms: Predictors of malignant and invasive pathology. Ann Surg 2007;246:644-51.
|
| 58. |
Nagai K, Doi R, Kida A, Kami K, Kawaguchi Y, Ito T, et al. Intraductal papillary mucinous neoplasms of the pancreas: Clinicopathologic characteristics and long-term follow-up after resection. World J Surg 2008;32:271-8.
|
| 59. |
Mimura T, Masuda A, Matsumoto I, Shiomi H, Yoshida S, Sugimoto M, et al. Predictors of malignant intraductal papillary mucinous neoplasm of the pancreas. J Clin Gastroenterol 2010;44:e224-9.
|
| 60. |
Crippa S, Fernández-Del Castillo C, Salvia R, Finkelstein D, Bassi C, Domínguez I, et al. Mucin-producing neoplasms of the pancreas: An analysis of distinguishing clinical and epidemiologic characteristics. Clin Gastroenterol Hepatol 2010;8:213-9.
|
| 61. |
Rodriguez JR, Salvia R, Crippa S, Warshaw AL, Bassi C, Falconi M, et al. Branch-duct intraductal papillary mucinous neoplasms: Observations in 145 patients who underwent resection. Gastroenterology 2007;133:72-9.
|
| 62. |
Jang JW, Kim MH, Jeong SU, Kim J, Park do H, Lee SS, et al. Clinical characteristics of intraductal papillary mucinous neoplasm manifesting as acute pancreatitis or acute recurrent pancreatitis. J Gastroenterol Hepatol 2013;28:731-8.
|
| 63. |
Capurso G, Boccia S, Salvia R, Del Chiaro M, Frulloni L, Arcidiacono PG, et al. Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: A multicentre case-control study. Am J Gastroenterol 2013;108:1003-9.
|
| 64. |
Hwang DW, Jang JY, Lim CS, Lee SE, Yoon YS, Ahn YJ, et al. Determination of malignant and invasive predictors in branch duct type intraductal papillary mucinous neoplasms of the pancreas: A suggested scoring formula. J Korean Med Sci 2011;26:740-6.
|
| 65. |
Bournet B, Kirzin S, Carrère N, Portier G, Otal P, Selves J, et al. Clinical fate of branch duct and mixed forms of intraductal papillary mucinous neoplasia of the pancreas. J Gastroenterol Hepatol 2009;24:1211-7.
|
| 66. |
Sugiyama M, Izumisato Y, Abe N, Masaki T, Mori T, Atomi Y. Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg 2003;90:1244-9.
|
| 67. |
Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, et al. Intraductal papillary mucinous neoplasms of the pancreas: An updated experience. Ann Surg 2004;239:788-97.
|
| 68. |
Lee SY, Lee KT, Lee JK, Jeon YH, Choi D, Lim JH, et al. Long-term follow up results of intraductal papillary mucinous tumors of pancreas. J Gastroenterol Hepatol 2005;20:1379-84.
|
| 69. |
Schnelldorfer T, Sarr MG, Nagorney DM, Zhang L, Smyrk TC, Qin R, et al. Experience with 208 resections for intraductal papillary mucinous neoplasm of the pancreas. Arch Surg 2008;143:639-46.
|
| 70. |
Ohno E, Hirooka Y, Itoh A, Ishigami M, Katano Y, Ohmiya N, et al. Intraductal papillary mucinous neoplasms of the pancreas: Differentiation of malignant and benign tumors by endoscopic ultrasound findings of mural nodules. Ann Surg 2009;249:628-34.
|
| 71. |
Nara S, Onaya H, Hiraoka N, Shimada K, Sano T, Sakamoto Y, et al. Preoperative evaluation of invasive and noninvasive intraductal papillary-mucinous neoplasms of the pancreas: Clinical, radiological, and pathological analysis of 123 cases. Pancreas 2009;38:8-16.
|
| 72. |
Suzuki Y, Atomi Y, Sugiyama M, Isaji S, Inui K, Kimura W, et al. Cystic neoplasm of the pancreas: A Japanese multiinstitutional study of intraductal papillary mucinous tumor and mucinous cystic tumor. Pancreas 2004;28:241-6.
|
| 73. |
Kanno A, Satoh K, Hirota M, Hamada S, Umino J, Itoh H, et al. Prediction of invasive carcinoma in branch type intraductal papillary mucinous neoplasms of the pancreas. J Gastroenterol 2010;45:952-9.
|
| 74. |
Sadakari Y, Ienaga J, Kobayashi K, Miyasaka Y, Takahata S, Nakamura M, et al. Cyst size indicates malignant transformation in branch duct intraductal papillary mucinous neoplasm of the pancreas without mural nodules. Pancreas 2010;39:232-6.
|
| 75. |
Jang JY, Kim SW, Lee SE, Yang SH, Lee KU, Lee YJ, et al. Treatment guidelines for branch duct type intraductal papillary mucinous neoplasms of the pancreas: When can we operate or observe? Ann Surg Oncol 2008;15:199-205.
|
| 76. |
Kim SC, Park KT, Lee YJ, Lee SS, Seo DW, Lee SK, et al. Intraductal papillary mucinous neoplasm of the pancreas: Clinical characteristics and treatment outcomes of 118 consecutive patients from a single center. J Hepatobiliary Pancreat Surg 2008;15:183-8.
|
| 77. |
Furukawa T, Klöppel G, Volkan Adsay N, Albores-Saavedra J, Fukushima N, Horii A, et al. Classification of types of intraductal papillary-mucinous neoplasm of the pancreas: A consensus study. Virchows Arch 2005;447:794-9.
|
| 78. |
Furukawa T, Hatori T, Fujita I, Yamamoto M, Kobayashi M, Ohike N, et al. Prognostic relevance of morphological types of intraductal papillary mucinous neoplasms of the pancreas. Gut 2011;60:509-16.
|
| 79. |
Mino-Kenudson M, Fernández-del Castillo C, Baba Y, Valsangkar NP, Liss AS, Hsu M, et al. Prognosis of invasive intraductal papillary mucinous neoplasm depends on histological and precursor epithelial subtypes. Gut 2011;60:1712-20.
|
| 80. |
Yamada S, Fujii T, Shimoyama Y, Kanda M, Nakayama G, Sugimoto H, et al. Clinical implication of morphological subtypes in management of intraductal papillary mucinous neoplasm. Ann Surg Oncol 2014;21:2444-52.
|
| 81. |
Kang MJ, Lee KB, Jang JY, Han IW, Kim SW. Evaluation of clinical meaning of histological subtypes of intraductal papillary mucinous neoplasm of the pancreas. Pancreas 2013;42:959-66.
|
| 82. |
Distler M, Kersting S, Niedergethmann M, Aust DE, Franz M, Rückert F, et al. Pathohistological subtype predicts survival in patients with intraductal papillary mucinous neoplasm (IPMN) of the pancreas. Ann Surg 2013;258:324-30.
|
| 83. |
Waters JA, Schmidt CM, Pinchot JW, White PB, Cummings OW, Pitt HA, et al. CT vs MRCP: Optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101-9.
|
| 84. |
Kawakubo K, Tada M, Isayama H, Sasahira N, Nakai Y, Takahara N, et al. Disease-specific mortality among patients with intraductal papillary mucinous neoplasm of the pancreas. Clin Gastroenterol Hepatol 2014;12:486-91.
|
| 85. |
Efthymiou A, Podas T, Zacharakis E. Endoscopic ultrasound in the diagnosis of pancreatic intraductal papillary mucinous neoplasms. World J Gastroenterol 2014;20:7785-93.
|
| 86. |
Lee KH, Lee SJ, Lee JK, Ryu JK, Kim EY, Kim TH, et al. Prediction of malignancy with endoscopic ultrasonography in patients with branch duct-type intraductal papillary mucinous neoplasm. Pancreas 2014;43:1306-11.
|
| 87. |
Pitman MB, Genevay M, Yaeger K, Chebib I, Turner BG, Mino-Kenudson M, et al. High-grade atypical epithelial cells in pancreatic mucinous cysts are a more accurate predictor of malignancy than “positive” cytology. Cancer Cytopathol 2010;118:434-40.
|
| 88. |
Sadot E, Basturk O, Klimstra DS, Gönen M, Anna L, Do RK, et al. Tumor-Associated Neutrophils and Malignant Progression in Intraductal Papillary Mucinous Neoplasms: An Opportunity for Identification of High-Risk Disease. Ann Surg 2015: Epub ahead of print. Vol OO, Number 00. pages 1-7.
|
| 89. |
Ohtsuka T, Matsunaga T, Kimura H, Watanabe Y, Tamura K, Ideno N, et al. Role of pancreatic juice cytology in the preoperative management of intraductal papillary mucinous neoplasm of the pancreas in the era of international consensus guidelines 2012. World J Surg 2014;38:2994-3001.
|
| 90. |
Hirono S, Tani M, Kawai M, Okada K, Miyazawa M, Shimizu A, et al. The carcinoembryonic antigen level in pancreatic juice and mural nodule size are predictors of malignancy for branch duct type intraductal papillary mucinous neoplasms of the pancreas. Ann Surg 2012;255:517-22.
|
| 91. |
Nagayoshi Y, Aso T, Ohtsuka T, Kono H, Ideno N, Igarashi H, et al. Peroral pancreatoscopy using the SpyGlass system for the assessment of intraductal papillary mucinous neoplasm of the pancreas. J Hepatobiliary Pancreat Sci 2014;21:410-7.
|
| 92. |
Goh BK, Tan DM, Ho MM, Lim TK, Chung AY, Ooi LL. Utility of the sendai consensus guidelines for branch-duct intraductal papillary mucinous neoplasms: A systematic review. J Gastrointest Surg 2014;18:1350-7.
|
| 93. |
Anand N, Sampath K, Wu BU. Cyst features and risk of malignancy in intraductal papillary mucinous neoplasms of the pancreas: A meta-analysis. Clin Gastroenterol Hepatol 2013;11:913-21.
|
| 94. |
Kim KW, Park SH, Pyo J, Yoon SH, Byun JH, Lee MG, et al. Imaging features to distinguish malignant and benign branch-duct type intraductal papillary mucinous neoplasms of the pancreas: A meta-analysis. Ann Surg 2014;259:72-81.
|
| 95. |
Fritz S, Klauss M, Bergmann F, Hackert T, Hartwig W, Strobel O, et al. Small (Sendai negative) branch-duct IPMNs: Not harmless. Ann Surg 2012;256:313-20.
|
| 96. |
Wong J, Weber J, Centeno BA, Vignesh S, Harris CL, Klapman JB, et al. High-grade dysplasia and adenocarcinoma are frequent in side-branch intraductal papillary mucinous neoplasm measuring less than 3 cm on endoscopic ultrasound. J Gastrointest Surg 2013;17:78-84.
|
| 97. |
Karachristos A, Esnaola NF. Surgical management of pancreatic neoplasms: What′s new? Curr Gastroenterol Rep 2014;16:397.
|
| 98. |
Aso T, Ohtsuka T, Matsunaga T, Kimura H, Watanabe Y, Tamura K, et al. “High-risk stigmata” of the 2012 international consensus guidelines correlate with the malignant grade of branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreas 2014;43:1239-43.
|
| 99. |
Kobayashi G, Fujita N, Maguchi H, Tanno S, Mizuno N, Hanada K, et al. Natural history of branch duct intraductal papillary mucinous neoplasm with mural nodules: A Japan Pancreas Society multicenter study. Pancreas 2014;43:532-8.
|
| 100. |
Ishikawa D, Shimada M, Utsunomiya T, Morine Y, Imura S, Ikemoto T, et al. Effect of Twist and Bmi1 on intraductal papillary mucinous neoplasm of the pancreas. J Gastroenterol Hepatol 2014;29:2032-7.
|
| 101. |
Ikemoto T, Sugimoto K, Shimada M, Utsunomiya T, Morine Y, Imura S, et al. Clinical role of Notch signaling pathway in intraductal papillary mucinous neoplasm of the pancreas. J Gastroenterol Hepatol 2015;30:217-22.
|
| 102. |
Kawakubo K, Tada M, Isayama H, Sasahira N, Nakai Y, Takahara N, et al. Risk for mortality from causes other than pancreatic cancer in patients with intraductal papillary mucinous neoplasm of the pancreas. Pancreas 2013;42:687-91.
|
| 103. |
Roch AM, DeWitt JM, Al-Haddad MA, Schmidt CM 2 nd , Ceppa EP, House MG, et al. Nonoperative management of main pancreatic duct-involved intraductal papillary mucinous neoplasm might be indicated in select patients. J Am Coll Surg 2014;219:122-9.
|
| 104. |
Sauvanet A, Gaujoux S, Blanc B, Couvelard A, Dokmak S, Vullierme MP, et al. Parenchyma-sparing pancreatectomy for presumed noninvasive intraductal papillary mucinous neoplasms of the pancreas. Ann Surg 2014;260:364-71.
|
| 105. |
Piciucchi M, Crippa S, Del Chiaro M, Valente R, Pezzilli R, Falconi M, et al. Outcomes of intraductal papillary mucinous neoplasm with “Sendai-positive” criteria for resection undergoing non-operative management. Dig Liver Dis 2013;45:584-8.
|
| 106. |
Salvia R, Fernández-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: Clinical predictors of malignancy and long-term survival following resection. Ann Surg 2004;239:678-85.
|
| 107. |
Marchegiani G, Mino-Kenudson M, Sahora K, Morales-Oyarvide V, Thayer S, Ferrone C, et al. IPMN involving the main pancreatic duct: Biology, epidemiology, and long-term outcomes following resection. Ann Surg 2014:00:1-8.
|
| 108. |
Kang MJ, Jang JY, Lee KB, Chang YR, Kwon W, Kim SW. Long-term prospective cohort study of patients undergoing pancreatectomy for intraductal papillary mucinous neoplasm of the pancreas: Implications for postoperative surveillance. Ann Surg 2014;260:356-63.
|
| 109. |
Larghi A, Panic N, Capurso G, Leoncini E, Arzani D, Salvia R, et al. Prevalence and risk factors of extrapancreatic malignancies in a large cohort of patients with intraductal papillary mucinous neoplasm (IPMN) of the pancreas. Ann Oncol 2013;24:1907-11.
|
| 110. |
Reddy S, Cameron JL, Scudiere J, Hruban RH, Fishman EK, Ahuja N, et al. Surgical management of solid-pseudopapillary neoplasms of the pancreas (Franz or Hamoudi tumors): A large single-institutional series. J Am Coll Surg 2009;208:950-7.
|
| 111. |
Butte JM, Brennan MF, Gönen M, Tang LH, D′Angelica MI, Fong Y, et al. Solid pseudopapillary tumors of the pancreas. Clinical features, surgical outcomes, and long-term survival in 45 consecutive patients from a single center. J Gastrointest Surg 2011;15:350-7.
|
| 112. |
Abraham SC, Klimstra DS, Wilentz RE, Yeo CJ, Conlon K, Brennan M, et al. Solid-pseudopapillary tumors of the pancreas are genetically distinct from pancreatic ductal adenocarcinomas and almost always harbor beta-catenin mutations. Am J Pathol 2002;160:1361-9.
|
| 113. |
Tanaka Y, Kato K, Notohara K, Hojo H, Ijiri R, Miyake T, et al. Frequent beta-catenin mutation and cytoplasmic/nuclear accumulation in pancreatic solid-pseudopapillary neoplasm. Cancer Res 2001;61:8401-4.
|
| 114. |
Igbinosa O. Pseudopapillary tumor of the pancreas. An algorithmic approach. JOP 2011;12:262-5.
|
| 115. |
Bostanoglu S, Otan E, Akturan S, Hamamci EO, Bostanoglu A, Gokce A, et al. Frantz′s tumor (solid pseudopapillary tumor) of the pancreas. A case report. JOP 2009;10:209-11.
|
| 116. |
Kamat RN, Naik LD, Joshi RM, Amrapurkar AD, Shetty TS. Solid pseudopapillary tumor of the pancreas. Indian J Pathol Microbiol 2008;51:271-3.
[PUBMED] |
| 117. |
Bouassida M, Mighri MM, Bacha D, Chtourou MF, Touinsi H, Azzouz MM, et al. Solid pseudopapillary neoplasm of the pancreas in an old man: Age does not matter. Pan Afr Med J 2012;13:8.
|
| 118. |
Law JK, Ahmed A, Singh VK, Akshintala VS, Olson MT, Raman SP, et al. A systematic review of solid-pseudopapillary neoplasms: Are these rare lesions? Pancreas 2014;43:331-7.
|
| 119. |
Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of the pancreas: Review of 718 patients reported in English literature. J Am Coll Surg 2005;200:965-72.
|
| 120. |
Yu PF, Hu ZH, Wang XB, Guo JM, Cheng XD, Zhang YL, et al. Solid pseudopapillary tumor of the pancreas: A review of 553 cases in Chinese literature. World J Gastroenterol 2010;16:1209-14.
|
| 121. |
Ansari D, Elebro J, Tingstedt B, Ygland E, Fabricius M, Andersson B, et al. Single-institution experience with solid pseudopapillary neoplasm of the pancreas. Scand J Gastroenterol 2011;46:1492-7.
|
| 122. |
Kang CM, Kim KS, Choi JS, Kim H, Lee WJ, Kim BR. Solid pseudopapillary tumor of the pancreas suggesting malignant potential. Pancreas 2006;32:276-80.
|
| 123. |
Martin RC, Klimstra DS, Brennan MF, Conlon KC. Solid-pseudopapillary tumor of the pancreas: A surgical enigma? Ann Surg Oncol 2002;9:35-40.
|
| 124. |
Tipton SG, Smyrk TC, Sarr MG, Thompson GB. Malignant potential of solid pseudopapillary neoplasm of the pancreas. Br J Surg 2006;93:733-7.
|
| 125. |
Mulkeen AL, Yoo PS, Cha C. Less common neoplasms of the pancreas. World J Gastroenterol 2006;12:3180-5.
 |
Authors
Tanima Jana, MD: Dr. Jana, Senior Resident, Department of Internal Medicine, The University of Texas Health Science Center, Houston, TX, USA
Jennifer Shroff, MD: Dr. Shroff, Assistant Professor, Department of Internal Medicine, Division of Gastroenterology, Hepatology, and Nutrition, The University of Texas Health Science Center, Houston, TX, USA
Manoop S. Bhutani, MD: Dr. Bhutani, Professor of Medicine and Cancer Systems, Imaging and Director of Endoscopic Research and Development, Department of Gastroenterology, Hepatology and Nutrition, UT MD Anderson Cancer Center, Houston, Texas, USA
Tables
[Table 1]